Absolutely (although I believe you meant in vivo; in vitro is in a petri dish).
Consider the Big 2 (Buhlmann+GFs and VPM). Buhlmann arbitrarily models 16 (12, 8) compartments, assumes that an exponential law governs ongasing and offgasing in each of these (the on/offgassing model) and further assumes a linear law specifies what minimum ambient pressure can be tolerated (the deco model). Testing was used to adjust all the constants to make the model "safe" (for a certain value of safe)(although ZHL16A used formulas to derive the a and b deco model constants from the on/offgasing model constants, if anyone knows how those formulas were arrived to, I'd be interested). GFs are just a dodgy hack to fix up the deco linear law to do deep stops (put down the flamethrower, that's what I'm diving too
). VPM uses bubble modeling for the deco model; the on/offgasing model is the same.
Yeah, blah blah blah, quite right, sorry. The point here is that none of that even pretends to describes what's happening to the body. Never mind a body in diving conditions, working, or not, getting cold, getting dehydrated and so on. Cheers,
Matthieu
This is a good topic, as I feel many with an interest in modelling, don't appreciate the relevance of this.
The Deco models in use today do not try to reproduce the physiology. Too many interested people fail to understand this. A deco model tries to model the danger zone and creates limits here.
It is currently impossible to reproduce the human circulation system in a math model. If such a thing was invented, it would be put to important use in medicine with the diagnosis of a 1000 human diseases and ailments.
Deco models are built around parameters we can measure in the water. That is: pressure and time. Many other variables affect the required deco time, but we can't measure or use them in a dive. As a diver in the water, we can only measure pressure and time which leaves very little for a deco model to work with.
If we could measure more variables, like body temp, circulation rates, and actual on / off gassing, then we could make our deco models more capable. For that I think we would need sensors and probes on the body, communicating to a computer. Now - here is the interesting part of such a capable model; For most of the dives we do, it would suggest LESS time than we do now. That's simply because our models and calibration we use today already have a safety buffer that fits the average diver and average situation. A more accurate model calculation would give less time. Are today's divers comfortable doing less time when its appropriate? Probably not.
As pointed out, many older models use only averages of time and pressure to track exposure. There are many versions of this approach - with a varying amount of cells in series or parallel. Then they typically apply a set of constant or factors to determine ascent limits. These simple model limits are fitted values to match observations. The problem here is the simple time + pressure averaging coupled with factors / constants, will quickly gets out of step with the physiology. Hence the GF is applied to patch up ZHL. RD uses several rule sets to compensate.
(Mark, this is why ZHL will never make you happy - the further you go to the extremes of the profiles, the further you venture from the fitted calibration zone).
Bubble models (VPM/RGBM) go one step further, by applying the science of microbubble behavior to the time / pressure averaging. All dives involve microbubbles, so it seems this approach is a lot closer to the physiology. Bubble models seem to span the diving spectrum without need for adjustment.
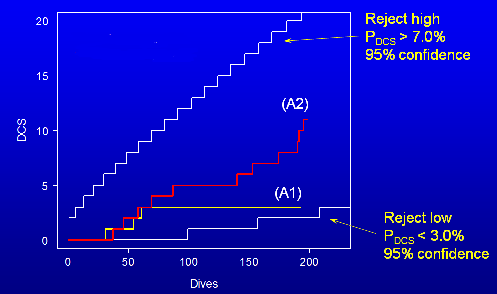
Another model concept that I thought showed promise was the DCIEM. Here they made ultrasound observations of microbubbles in test dives. From that they created tables that gave consistent levels of microbubbles. Interestingly, this also aligns nicely with the bubble model approach too.
Regards rossh
Last edited: