UWSojourner
Active Member
There is nothing "self appointed" about my expertise Ross. I am happy to let people judge that for themselves based on my CV.
The thud you heard is Dr. Mitchell dropping the mic on Ross' silliness.

Last edited:
There is nothing "self appointed" about my expertise Ross. I am happy to let people judge that for themselves based on my CV.
If only he'd stop publishing so much he'd have time to validate "his" decompression theoriesThe thud you heard is Dr. Mitchell dropping the mic on Ross' silliness.
View attachment 10084

Ross, I don't claim to be a decompression theorist, but I am having a difficult time understanding your reasoning with this comment. Surely, supersaturation is an issue regardless of whether it is present during the dive or afterwards. Do you not feel that things such as altitude changes, workload, surface O2 use, etc. come into play while on the surface or are you trying to say that anything that impacts decompression happens during the dive? If this is indeed what you are trying to say, it would seem to fly in the face of all decompression training I have ever received.
If I have misunderstood your statement, can you please clarify what you mean by "controlling the dive supersaturation is the only dimension that matters."?
These guys are busy trying to push through yet another fake measure, with no actual validation to their claims of stress and risk relevance.. Why are you allowing them to get away with this?
******
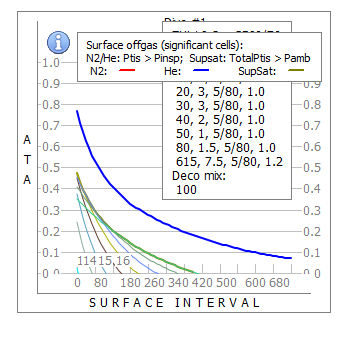
This is surface decompression from Don's dives. legend: Blue / red line is the off gas gradient of He / N2. The gold line is the current supersaturation level. The patchwork underneath it is the trace line for each individual cell. That patchwork of overlapping and unconnected values is what Kevin is adding up into one giant number for his surface value.
Don's surface supersaturation.
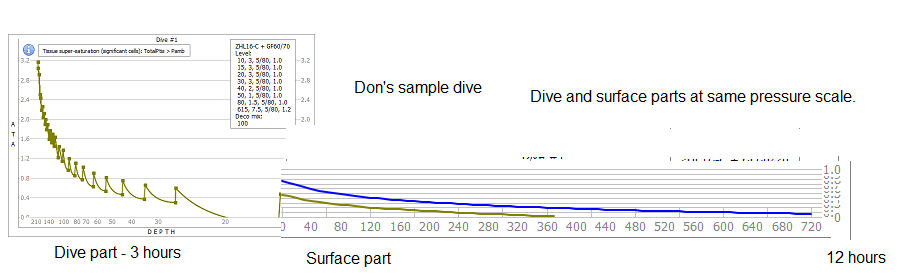
Don's dive with both surface and dive parts drawn at the same pressure scale, we have connected them together as one continuous piece.
Note how the dive part is clearly the most significant component. The surface part is a follow on and secondary consideration. For any given dive the only control we get for the surface supersaturation, is the placement of the initial start point height. When you hit the surface, all saturation pressures are in rapid decline. This is why the last stop time is very flexible in practice.
But Kevin/ Simons junk science ISS draws the surface part bigger. From a stress /risk perspective (that they claim to represent), that difference is obviously wrong.
*************
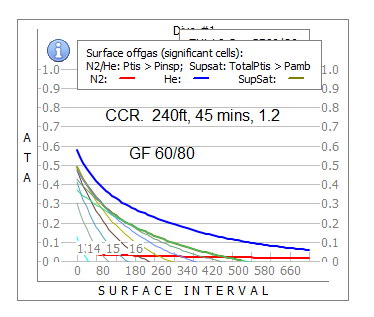
Surface supersaturation from various dives. Note how it gets bigger with every dive size.
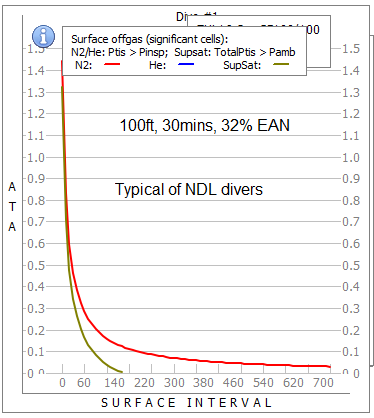
This is a recreational deco dive. The surface supersaturation is typical of NDL divers. You can see his supersaturation is all gone within 2.5 hours. But this group of divers are very good at making overnight DCS injuries (12 hours). If supersaturation was the cause here, then it has to happen very early...OR..... what else could be the cause????
The 'typical UK channel' dive.. supersaturation lasts about 9 hours.
***************
Does small differences in surface supersaturation matter? No. Clearly the deco diver has magnitudes more surface supersaturation than of the NDL diver. They both get DCS though.
Does the absolute value of surface supersaturation matter? No. The real concern for pressure values is what occurs in the dive deco part.
Obviously the dive part is the most serious concern for supersaturation, and surface supersaturation is a secondary issue, which under normal conditions is not important to the outcome.
It should have become obvious to readers, the the Kevin / Simon giant number ISS is not going to work.. Decompression risk / stress is more complicated than their simplistic method which is often wrong for the results they claim..
.
This explanation was actually beneficial to see. I had been wondering what you meant by "overlapping and unconnected" compartments. Now I know. A compartment is "overlapping and unconnected" if the lines overlap on Ross's line plot of compartment supersaturation. I'm still laughing.This is surface decompression from Don's dives. legend: Blue / red line is the off gas gradient of He / N2. The gold line is the current supersaturation level. The patchwork underneath it is the trace line for each individual cell. That patchwork of overlapping and unconnected values is what Kevin is adding up into one giant number for his surface value.
It would be preferable if you actually reviewed what was posted. If you'd simply checked the ISS chart I posted earlier you would see that Don's GF 60/84 profile had higher ISS for the dive portion of the planned dive. The ISS for the "fast ascent" profile with GF60/69 is shown below . Note the green bars "In water" and "On surface". The "in water" component is indeed larger.Don's surface supersaturation .... Note how the dive part is clearly the most significant component.

It's clearly more of a secondary consideration for the GF profile (green bars) than the VPM-B profile (red bars). Remember this is the profile where VPM-B surfaces the diver at a GF in excess of 130. Try as you might Ross -- not many divers are going to see surfacing at a GF in excess of 130 as a "secondary consideration". And I think it's relatively easy to see why VPM-B's surface portion of the dive would be higher stress, as is indicated by the ISS chart, since VPM-B is booting the diver onto the surface with a GF over 130, and compartments 9-16 all over GF 100 -- high stress indeed.The surface part is a follow on and secondary consideration.
This would really be funny if it weren't so pitiful.Does the absolute value of surface supersaturation matter? No.
Ross - perhaps you should invest some time in means, mode and median for measures of centrality. They suffer in a similar way to ISS in that they take a data set and give you a single number. Two different data sets may have the same mean but very different modes or medians. In fact it’s rare to give a measure of centrality without a measure of spread like confidence intervals or standard deviations. In summary reducing data to a single point has merit and short falls - there is no conspiracy theory
The patchwork underneath it is the trace line for each individual cell. That patchwork of overlapping and unconnected values is what Kevin is adding up into one giant number for his surface value.
Don's dive with both surface and dive parts drawn at the same pressure scale, we have connected them together as one continuous piece.
Note how the dive part is clearly the most significant component.
The surface part is a follow on and secondary consideration. For any given dive the only control we get for the surface supersaturation, is the placement of the initial start point height. When you hit the surface, all saturation pressures are in rapid decline.
Surface supersaturation from various dives. Note how it gets bigger with every dive size.
and...
Does small differences in surface supersaturation matter? No. Clearly the deco diver has magnitudes more surface supersaturation than of the NDL diver. They both get DCS though.
This is a recreational deco dive. The surface supersaturation is typical of NDL divers. You can see his supersaturation is all gone within 2.5 hours. But this group of divers are very good at making overnight DCS injuries (12 hours). If supersaturation was the cause here, then it has to happen very early...OR..... what else could be the cause????
Does the absolute value of surface supersaturation matter? No. The real concern for pressure values is what occurs in the dive deco part.
Obviously the dive part is the most serious concern for supersaturation, and surface supersaturation is a secondary issue, which under normal conditions is not important to the outcome.
I think you should at least ask yourself "What is the alternative?" Ross unopposed?Why do I have the feeling that this thread degenerated to a cockfight shortly after Ross and Simon started posting. For at least the last 6 weeks there hasn't been anything posted that could possibly help Don with his DCS.
Either put Ross and Simon in a cockfighting ring chained to each other on their left hands with a Bowieknife each until only one is still bleeding, or make each of them prepay $10 per posting in the future in order to post.
Michael
I think you should at least ask yourself "What is the alternative?" Ross unopposed?
Labeling Dr. Mitchell's involvement in this thread as a "cockfight" between him and Ross would be similar to saying an arsonist and a firefighter are a couple of guys creating a big mess. While nobody disputes the mess, implying such equivalency misses the heart of what occurred.
What exactly is your point about the "patchwork of overlapping and unconnected values" that "Kevin is adding up into one giant number for his surface value"?
As Kevin has explained above, with reference to David's comments on the matter, if a notional tissue represented by one of those lines is supersaturated, then it could form bubbles, and could therefore contribute to risk of developing DCS symptoms. You have lots of tissues that are supersaturated to differing degrees depicted in your graph. It doesn't matter a damn whether their supersaturation values are the same or different of "overlap" or whatever. All could form bubbles and therefore contribute to the risk of developing symptoms. Under these circumstances, why would you consider some tissues but ignore others, which seems to be a belief of yours?
If you can't accept this, then I would simply say too bad. You are manufacturing an anti-ISS narrative that blatantly ignores a mass of evidence that ISS can be calibrated for use in prediction of risk in probabilistic decompression models as Dr Doolette has told you. Put simply, it is a useful index of risk. Your manufactured narrative includes an allusion to ISS calculated by UWSojourner somehow being different to ISS calculated by other decompression modellers. Dr Doolette has also told you this is incorrect. Nobody is claiming ISS is the only factor determining risk but when comparing risk in two decompression approaches of the same length from the same dive, it is a very useful index.
Leaving aside the fact that this is Don's dive and that his ascent rate was too fast, your diagram does NOT demonstrate that “the dive part is clearly the most significant component”. The diagram is a deceptive depiction of the process, and it relies on an assumption that all supersaturation in all tissues is equal in terms of its pathophysiological significance. That is not true, or at the very least, it is certainly not how most approaches to decompression interpret it. As you well know, Buhlmann and GF approaches allow more supersaturation in fast tissue early because it is assumed that fast tissues tolerate it better than slower tissues. Hence, a depiction of a shallower stop approach to decompression will always look like the one you have posted above with a higher spike in faster tissue supersaturation early.
However, and this cycles us right back to the start of this debate (years ago) the evidence from all the comparative humans studies conducted to date suggests that reducing the fast tissue supersaturation spike early in the dive by using excessive deep stops, at the expense of a much more subtle looking increase in slow tissue supersaturation later in the ascent and at the surface is associated with worse outcomes. It follows that your depiction above is completely unsuited to the purpose of illustrating where harmful supersaturation occurs, or which part of an ascent and surface continuum is more important.
Of course supersaturation is declining at the surface. Its called outgassing. But so what? In an earlier post you advanced the ridiculous notion that this creates a good environment for microbubble dissolution despite there being copious evidence (cited in an earlier post of mine) that bubble formation accelerates after surfacing. You said that this creates a milieu "favourable to tissue micro-bubble reduction" in this latest post too, but you have edited it out (presumably because you have thought about it and come to the conclusion that it is wrong?). So if that is wrong, what is your point about declining supersaturation? It is still potentially harmful even if it is declining.
What an extraordinarily naïve comment. Yes DCS can occur in both settings, but your implication that this proves surface supersaturation doesn't matter is patently nonsensical. You completely ignore the near certainty that the risk of DCS is greater with bigger "dive size" too. A recent study (currently in review) conducted in our temperate water environment showed a DCS rate of around 0.5:10,000 dives in scuba air no decompression divers. [1] A PDE subset from scapa flow where deeper dives and more decompression dives were done showed a DCS rate of 28 per 10,000 dives. [2] The scapa flow dives were in water that is colder for much of the year, and it is difficult to separate out the effects of the various risk factors but "dive size" was almost certainly part of it. So, in fact, it is exactly as we would expect: bigger "dive size" = more surface supersaturation = greater risk.
I have to say Ross, even a small indulgence in scholarly effort would save you a lot of embarrassment and prevent the dissemination of inaccurate information. The fact is that the vast majority of DCS cases in NDL dives arise exactly when you would expect them to on the bases of surface supersaturation driving bubble formation. Here are some examples from studies where the vast majority of the dives were NDL scuba air:
Blatteau et al: The median time from surfacing to onset of initial symptoms was 30 min. (279 cases of neurological DCS) [3]
Grover et al: The overwhelming majority of neurological DCS occurs within 2 hours of a dive. (review of many articles) [4]
Haas et al: Symptom onset ranged from “present on surfacing” to 168 hours after diving, with a median time of 1.5 hours (>500 mainly mild cases) [5]
Mitchell and Doolette: 85.4% presented within 60 minutes of surfacing. (239 cases of inner ear DCS) [6]
Yes, some "cases" have apparently delayed onset, but the vast majority of these are mild, and there is typically either a precipitating reason (such as ascent to altitude or flying) or a suspicion that the symptoms have been present for much longer than the diver admits (because the diver is trying to avoid being judged for failure to present earlier).
Arguably your most misguided and dangerous statements to date. Undeniable evidence that you have no place misrepresenting yourself as an expert in this area.
Simon M
1. Hubbard M, Davis M, Malcolm K, Mitchell SJ. Decompression illness and other injuries in a recreational dive charter operation. Diving Hyperb Med 2018 (under review).
2. Vann RD, Denoble PJ, Uguccioni DM, Pollock NW, Freiberger JJ, Pieper CF, et al. The risk of decompression sickness is influenced by dive conditions. Diving for Science 2005. Proceedings of the American Academy of Underwater Sciences. American Academy of Underwater Sciences; 2005.
3. Blatteau JE, Gempp E, Simon O, Coulange M, Delafosse B, Souday V et al. Prognostic factors of spinal cord decompression sickness in recreational diving: retrospective and multicentric analysis of 279 cases. Neurocrit Care. 2011;15:120-7.
4. Grover I, Reed W, Neuman T. The SANDHOG criteria and its validation for the diagnosis of DCS arising from bounce diving. Undersea Hyperb Med 2007;34:199-210
5. Mitchell SJ, Doolette DJ. Pathophysiology of inner ear decompression sickness: potential role of the persistent foramen ovale. Diving Hyperbaric Med 45, 105-110, 2015
6. Haas RM, Hannam JA, Sames C, Schmidt R, Tyson A, Francombe M, Richardson D, Mitchell SJ. Decompression illness in divers treated in Auckland, New Zealand 1996-2013. Diving Hyperbaric Med, 44, 20-25, 2014
Now go do it properly with independent validations, studies and proper peer reviewed reporting.
.
Where is yours?
Of what? I'm NOT the one trying to push new deco stress measures.. that's Kevin and Simon trying to convince you their ISS is reliable and can be trusted without any proper validations or independent analysis or reporting.
And then we have Simon's reinterpretations of science test papers to suit his arguments...... these guys are trying to cheat the system (again) and get away with another fait accompli. Don't let em get away with it.
Of what? I'm NOT the one trying to push new deco stress measures.. that's Kevin and Simon trying to convince you their ISS is reliable and can be trusted without any proper validations or independent analysis or reporting. And then we have Simon's reinterpretations of science test papers to suit his arguments...... these guys are trying to cheat the system (again) and get away with another fait accompli. Don't let em get away with it.
.
Right.
So ISS is
the integral for time between 0 (start of the dive) and infinity of
the sum for each compartment of
pComp,N2 + pComp,He - pAmbient if pComp,N2 + pComp,He - pAmbient > 0
0 otherwise
There is no arbitrary constant in there that would require justification or calibration.
At the very most one might suggest that treating all compartments equally might not be optimal. But the complete absence of constants at least has the virtue of making it clear that the metric was not tuned to advantage one profile over another.
Furthermore neither UWSojourner, nor Simon Mitchell, nor in fact anybody else has suggested any sort of limit above which a serious risk exists, which would also require justification or calibration.
On the other hand, you, in this very thread, in fact in this post, in effect, use the metric
the integral for time between 0 and infinity of
the maximum for each compartment of
1 if pComp,N2 + pComp,He - pAmbient > 2 bar (deemed "excessive")
0 otherwise
With the 2 bar threshold conveniently taken so that VPM profiles stay under it. Note that this metric also treats all compartments equally.
You further state that "The 7 mins above 2.0 is a major concern for any dive". Never justifying, much less "calibrating", either the 2 bar or the 7 minutes.
It beggars belief that you would demand that ISS be "calibrated", even though it is not required (at least for the usage that is made of it), while not doing it for your own metric, even though it does require it.
It becomes surreal that you would now claim that "they" only are pushing new metrics.
Matthieu
Nobody is trying to push a new deco stress measure. We are applying one that is extensively used. See this post from Dr Doolette to you here. Among other things, he says:
You state, in the legend of your figure nedu_pg2a_50.jpg in post #388, “Integral supersaturation is not a recognized, or verified, or useful measure in decompression.” This is just wrong. The integral supersaturation is the essence of many U.S. Navy probabilistic decompression models, there must be at least 30 research reports describing how such models provide good descriptions of the incidences of DCS in large data bases of dive profiles and known DCS outcomes, and such a model underlies the extensively validated U.S. Navy MK 16 MOD 1 He-O2 decompression tables.
But this is like so many things in these discussions. When an evidence-based point is made that discredits your position, you just flat out say its wrong; irrespective of how much hard evidence there is in support of it. Its unbelievable really - like a different parallel reality. As such you represent a massive impediment to the dissemination of accurate information in the diving community.
I am citing the scientific literature to back up the things I am saying. I'm not sure what else I am supposed to do. If you think I am citing the literature incorrectly, please point out why.
Simon M
That's not all that has been provided on the topic, but this "friend" of Dr. Mitchell's is a recognized decompression expert (and you are not). So his testimony on the matter matters.so far, you are just grabbing at quotes off the internet, all written by your friend, that amount to nothing that give any validation or authenticates your home made ISS version.
.
The 2 ATA value is a common limit value to diving research. Haldane used it in some of his initial work. If you do a survey of many model outputs, you will find most do not exceed 2 ATA, and certainly not for the first 300 ft of dive depths where most models work well. 2 ATA is an arbitrary number, but it's a sensible and well proven value. If you look deeper into the stop patterns of any model, you will find they almost all come well under the 2 ATA value. So 2 ATA is not my metric, but simply a common limit used throughout diving.
Your summation of ISS is correct, but Kevin does more than that, which makes his version unique.
Kevin / Simon ISS adds all the cells into one number. These overlapping values are against the rules of parallel model design (ZHL). Only serial models can add adjacent cell values, so he is compounding the same data. The stress represented in cell #10 (or any cell for that matter), cannot be added to the stress in any other adjacent cell, as stress in tissue x has no knowledge of stress in tissue y. Stress cannot be summed across the cells of a parallel model.
Then you have to decide if simplistic 'pressure x time' is appropriate, given that 'pressure to risk' is not a linear relationship. example 100 mins at 0.3 ATA, is harmless while 10 mins x 3.0 ATA is a serious risk, but they have the same ISS value. Clearly the risk scale needs a factor / exponential applied to bring stress / risk assessments in line with reality.
Next problem to solve - how does stress accumulated at say 5ATA depth, relate to stress on the surface? How to transpose whole dive stress into one common pressure scale? Obviously a stress and tissue bubble that started at 5ATA depth with 1 ATA supersaturation, and grew threw Boyles law, time and ascent from 5 to 1 ATA, represents a higher stress than a new 1 ATA stress recorded at the surface. This is why dive stress is far more important than surface stress.
I don't have the answer, and neither does Kevin / Simon. The deco stress problem is far more complex than simplistic ISS. If deco was that easy to solve then we could do away with deco models. Haldane tried it once.