Why would any GF that is less than 100/100 allow such overpressure, or any overpressure for that matter?
Yeah, so there's a few important points to consider when considering this "supersaturation pressure".
One, a compartment is not a tissue. A compartment, and its pressure, are abstractions. In this case, the classical exponential compartment is taken to be an idealised tissue such that:
- its content is homogeneous; in particular any concentration/pressure is the same everywhere.
- its only interface with the outside world is via the capillaries (*cough* lymphatic system *cough*).
- this interface is perfect: on leaving the compartment, the blood is at equilibrium with the compartment.
There's other simplifications, including about what happens in the lungs, but the key thing is that by making these assumptions, we don't have to deal with Fick's second law, a.k.a the heat equation. This is important because it's notoriously hard to solve exactly. As in, you can count the problems we can solve exactly on your fingers. Mostly, this is the realm of computers - real ones. It's less a case of neglecting stuff we know not to be relevant with the happy consequence that the math gets easier without changing the result, and more a case of removing difficulties until the math is tractable at all and hope for the best. That joke about a guy looking for his keys under the street light because that's where there's light comes to mind. Luckily enough, in diving applications, when we use a lot of these in parallel, we get a pretty good representation of what's happening to the whole body. That should not be taken to mean that those compartments and compartment pressures are a physical reality.
The bottom line is that care must be taken not to assign too much significance to arbitrary figures plucked out of the model. To stay with the streetlight joke, with enough streetlights you can model daytime pretty well, but that doesn't mean that if someone in a specific spot get blinded he'd also get blinded there in daylight.
Two, how helium is treated is... sloppy. It's taken to be dissolving faster because of its higher diffusivity. Well, maybe. But in our assumptions above, we've taken the whole compartment to be uniform, or, equivalently, diffusivities are taken to be infinite. We specifically avoided Fick's laws. So it's a bit of a fudge to reintroduce this through the backdoor "just because". That doesn't mean it's wrong, but one needs to bear this in mind. As it happens, there is experimental evidence that it is, in fact, wrong, at least for the faster tissues.
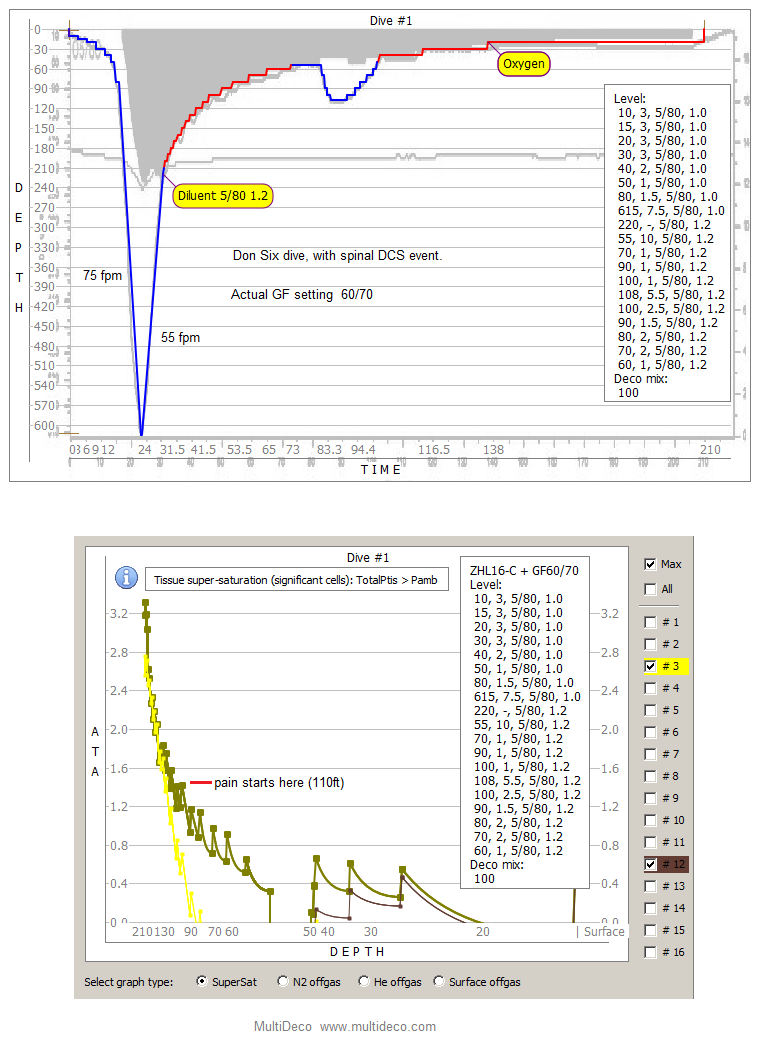
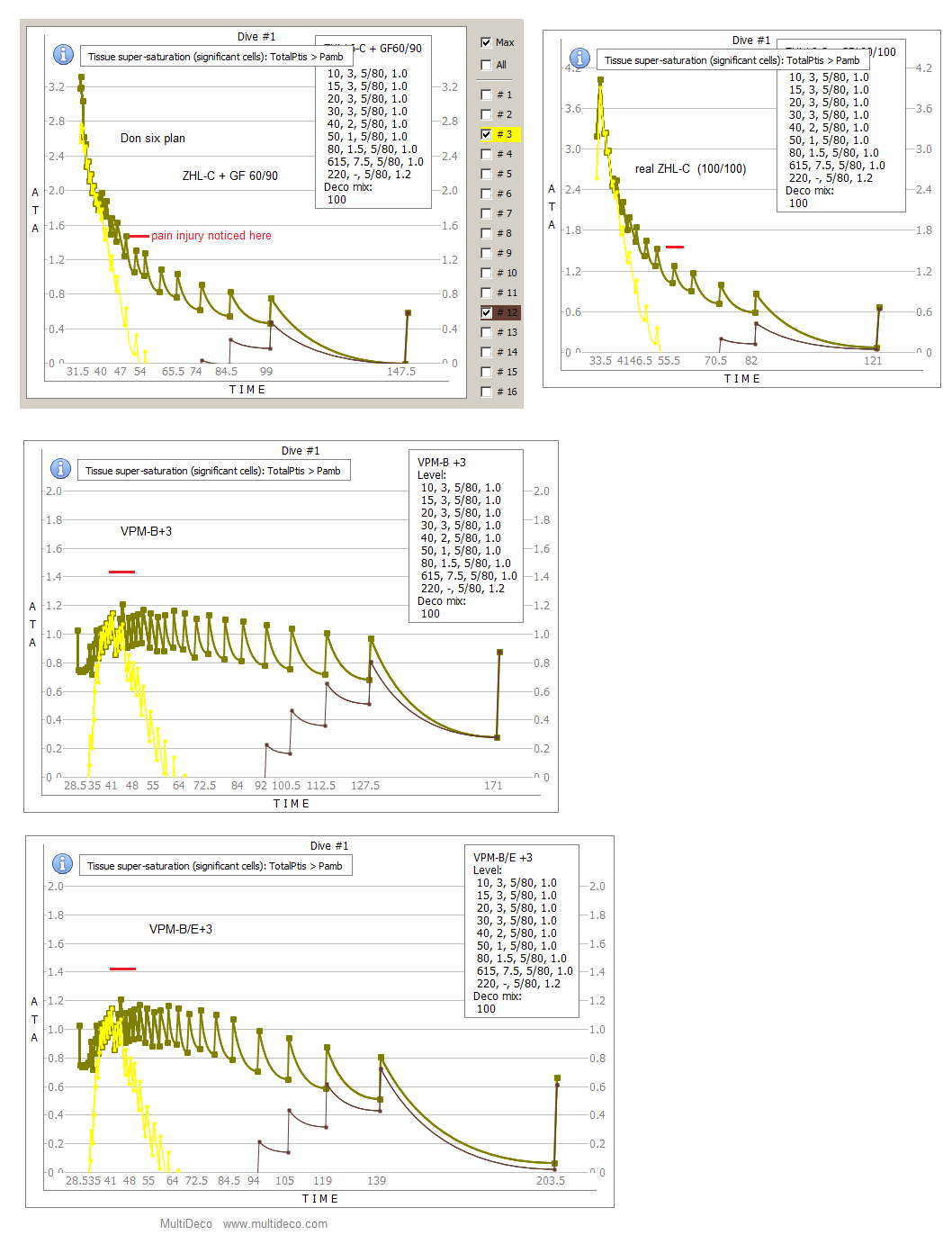
Three, Haldanian models take it that the allowed overpressure increases linearly with depth. So it should not be a surprise that GF 60/90 allows an overpressure at 66m (220') higher than what would on the surface be considered a "go straight to the chamber" situation. That's what they do.
As an aside, SurDO2 (that's Surface Decompression, FWIW) does not specify a "max pressure". That would make little sense for the reason stated above. What it says is finish your 40' stop, then you have 5 minutes to be in the pot.
Cheers,
Matthieu