You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
My DCS Hit
- Thread starter DSix36
- Start date
- Status
- Not open for further replies.
So Don, do you feel that the pain in the sternum you were experiencing at depth is related to your DCS hit?
DSix36
Well-Known Member
Myself and DAN do not believe it was the direct cause. The current belief is that it was the beginning of a cascade of events that added to the cause. Hard breathing caused the pain which later caused me to fully relax and thus no longer offgas as effectively. I have no doubt that it was part of the problem at the very least.So Don, do you feel that the pain in the sternum you were experiencing at depth is related to your DCS hit?
DSix36
Well-Known Member
Thanks for your report.
Do you know the default cracking pressure for your ADV and what the cracking pressure that you have it set at?
Have you altered your rEvo? in anyway that would have increased its stock WOB? ie. added a Shrimp BOV etc or moved it further off your back...
Not really a cracking pressure issue since it works via a plunger system directly on the interior of the counter lung, but no I do not know the default.
My rEvo is highly modified. The loop hoses are from Golem Gear and the DSV is from a Meg. It is one of the very first rEvo II's and only has part of the WOB kits installed. I kept the 90 degree p-port connectors for the loop because I do not like the straight ones on my unit.
Mike Ferguson
WTF is that?
Thanks for sharing and I'm glad to hear you're on the mend.
Sometimes shit happens and stories like this are a good reminder that all this deco theory is theory and that it really doesn't matter what your computer is saying when the model doesn't know that the squidgy biology isn't working as it should. Some days you get away it, some days you don't. Do enough dives and the chances of it not being your lucky day seem to increase. Though no doubt some muppet will be along shortly to tell you what you did 'wrong' and how they would never do that.
I'd be really interested to hear what you'd do differently if you ever feel like posting it as obviously you are the guy who knows the full details of the dive and the one who has had the time to run through the what if's and why did I do that?
One thing that did I did wonder about in your story was the GF 60/90. If you don't mind me asking, what drove the choice of GF 60/90? is this the usual GF you run with or something different for this dive?
Sometimes shit happens and stories like this are a good reminder that all this deco theory is theory and that it really doesn't matter what your computer is saying when the model doesn't know that the squidgy biology isn't working as it should. Some days you get away it, some days you don't. Do enough dives and the chances of it not being your lucky day seem to increase. Though no doubt some muppet will be along shortly to tell you what you did 'wrong' and how they would never do that.
I'd be really interested to hear what you'd do differently if you ever feel like posting it as obviously you are the guy who knows the full details of the dive and the one who has had the time to run through the what if's and why did I do that?
One thing that did I did wonder about in your story was the GF 60/90. If you don't mind me asking, what drove the choice of GF 60/90? is this the usual GF you run with or something different for this dive?
DSix36
Well-Known Member
Thanks for sharing and I'm glad to hear you're on the mend.
Sometimes shit happens and stories like this are a good reminder that all this deco theory is theory and that it really doesn't matter what your computer is saying when the model doesn't know that the squidgy biology isn't working as it should. Some days you get away it, some days you don't. Do enough dives and the chances of it not being your lucky day seem to increase. Though no doubt some muppet will be along shortly to tell you what you did 'wrong' and how they would never do that.
I'd be really interested to hear what you'd do differently if you ever feel like posting it as obviously you are the guy who knows the full details of the dive and the one who has had the time to run through the what if's and why did I do that?
One thing that did I did wonder about in your story was the GF 60/90. If you don't mind me asking, what drove the choice of GF 60/90? is this the usual GF you run with or something different for this dive?
60/90 is my normal GF
This story is a sober reminder of just how dangerous our weekend fun activity can get. I hope you have a full recovery.
************
Now to the analysis:
The choice of ZHL-C with GF 60/90 and a fast(ish) ascent rate, has given the following conditions:
It ascended through 11 ATA, while reaching and maintaining a supersaturation pressure of 3.3 ATA, for at least 8 mins. The supersaturation remained over 2 ATA for another 4 mins during the initial stops. That is a lot, and is typical of divers making a missed deco direct ascents.
If you want something valid to compare with: The USN SurD diver will typically endure 3.5 ATA supersaturation for a max time of 3 1/2 mins during the surface transfer, after which the chamber re-compression puts them back at around 1.5 ATA supersaturation. If they reach or exceed 5 mins during the surface time, then it becomes a DCS treatment process.
You have exceeded all those numbers by quite some margin.
Take a look:
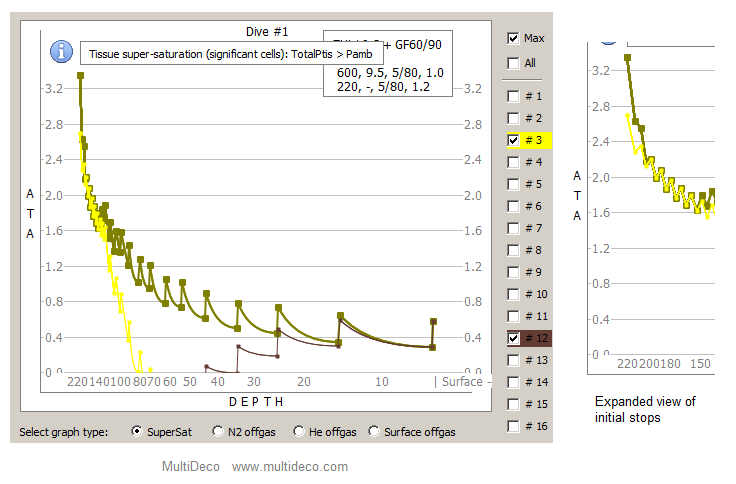
I have highlighted the fast cell # 3. This remained supersaturated up to, and beyond the point where you noticed the onset of injury, Conversely, the slower tissues did not reach supersaturated state until the 40 ft level.
Do I need to say it? Your choice of deco parameters and the depth combination, has exceeded the abilities of simple model you used. Perhaps a better choice would have been a model that is designed around the dynamics of depth and bubble growth.
.
************
Now to the analysis:
The choice of ZHL-C with GF 60/90 and a fast(ish) ascent rate, has given the following conditions:
It ascended through 11 ATA, while reaching and maintaining a supersaturation pressure of 3.3 ATA, for at least 8 mins. The supersaturation remained over 2 ATA for another 4 mins during the initial stops. That is a lot, and is typical of divers making a missed deco direct ascents.
If you want something valid to compare with: The USN SurD diver will typically endure 3.5 ATA supersaturation for a max time of 3 1/2 mins during the surface transfer, after which the chamber re-compression puts them back at around 1.5 ATA supersaturation. If they reach or exceed 5 mins during the surface time, then it becomes a DCS treatment process.
You have exceeded all those numbers by quite some margin.
Take a look:
I have highlighted the fast cell # 3. This remained supersaturated up to, and beyond the point where you noticed the onset of injury, Conversely, the slower tissues did not reach supersaturated state until the 40 ft level.
Do I need to say it? Your choice of deco parameters and the depth combination, has exceeded the abilities of simple model you used. Perhaps a better choice would have been a model that is designed around the dynamics of depth and bubble growth.
.
Last edited:
DSix36
Well-Known Member
This story is a sober reminder of just how dangerous our weekend fun activity can get. I hope you have a full recovery.
************
Now to the analysis:
The choice of ZHL-C with GF 60/90 and a fast(ish) ascent rate, has given the following conditions:
It ascended through 11 ATA, while reaching and maintaining a supersaturation pressure of 3.3 ATA, for at least 8 mins. The supersaturation remained over 2 ATA for another 4 mins during the initial stops. That is a lot, and is typical of divers making a missed deco direct ascents.
If you want something valid to compare with: The USN SurD diver will typically endure 3.5 ATA supersaturation for a max time of 3 1/2 mins during the surface transfer, after which the chamber re-compression puts them back at around 1.5 ATA supersaturation. If they reach or exceed 5 mins during the surface time, then it becomes a DCS treatment process.
You have exceeded all those numbers by quite some margin.
Take a look:
I have highlighted the fast cell # 3. This remained supersaturated up to, and beyond the point where you noticed the onset of injury, Conversely, the slower tissues did not reach supersaturated state until the 40 ft level.
Do I need to say it? Your choice of deco parameters and the depth combination, has exceeded the abilities of simple model you used. Perhaps a better choice would have been a model that is designed around the dynamics of depth and bubble growth.
.
I do not see where you incorporated the IWR change in depth and ascent timing. Did I miss something?
I do not see where you incorporated the IWR change in depth and ascent timing. Did I miss something?
I did not show that yet. The profile above is built on the information provided. If you have more details I can add the extra complexities. PM me with the info please.
Your follow up and recovery reads much like a spinal injury. By your own account, the spinal injury aspect was well formed by the time you realized it at 50ft, so this would seem to be an early onset "in water DCS" event.
The area I wish to highlight, is the ascent phase from 600ft to 220 ft, or 11 ATA, and how that over pressure event compares to a USN SurD over-pressure conditions and there limits.
Can I ask is this your personal opinion only or do you possess medical qualifications in this area that would support your prognosis.I did not show that yet. The profile above is built on the information provided. If you have more details I can add the extra complexities. PM me with the info please.
Your follow up and recovery reads much like a spinal injury. By your own account, the spinal injury aspect was well formed by the time you realized it at 50ft, so this would seem to be an early onset "in water DCS" event.
The area I wish to highlight, is the ascent phase from 600ft to 220 ft, or 11 ATA, and how that over pressure event compares to a USN SurD over-pressure conditions and there limits.
The spinal injury argument seems pretty non-controversial given both the IW symptoms and afterwards.
http://www.rebreatherworld.com/showthread.php?55323-My-DSC-Hit
I have no basis to comment on the SurD limits/tolerances and their relevance here.
http://www.rebreatherworld.com/showthread.php?55323-My-DSC-Hit
I have no basis to comment on the SurD limits/tolerances and their relevance here.
First off, thanks for sharing this.
Completely agree. I'd go a bit further about the relevance, though.
We have a diver who experienced two instances of "mild" chest pain in the final stages of his descent. This remained a "minor uncomforting feeling" from 600' to 110'. Then suddenly "extreme pain" at 110'. "Diminishing" from 110' to 50', where the diver realised he was bent.
Now I have no idea what caused the chest pain. While inhaling extremely forcefully? Something to do with the pleural cavity? I have no idea. I does however seem reasonable to imagine that lung function may have become compromised at this point. So offgasing was possibly hindered from 600' to 110', and definitely hindered from 110' to 50', because in addition the diver was now breathing shallow to relieve the pain.
It seems a bit... bizarre to completely ignore all this and focus on the deco model.
Cheers,
Matthieu
The spinal injury argument seems pretty non-controversial given both the IW symptoms and afterwards.
http://www.rebreatherworld.com/showthread.php?55323-My-DSC-Hit
I have no basis to comment on the SurD limits/tolerances and their relevance here.
Completely agree. I'd go a bit further about the relevance, though.
We have a diver who experienced two instances of "mild" chest pain in the final stages of his descent. This remained a "minor uncomforting feeling" from 600' to 110'. Then suddenly "extreme pain" at 110'. "Diminishing" from 110' to 50', where the diver realised he was bent.
Now I have no idea what caused the chest pain. While inhaling extremely forcefully? Something to do with the pleural cavity? I have no idea. I does however seem reasonable to imagine that lung function may have become compromised at this point. So offgasing was possibly hindered from 600' to 110', and definitely hindered from 110' to 50', because in addition the diver was now breathing shallow to relieve the pain.
It seems a bit... bizarre to completely ignore all this and focus on the deco model.
Cheers,
Matthieu
We have a diver who experienced two instances of "mild" chest pain in the final stages of his descent. This remained a "minor uncomforting feeling" from 600' to 110'. Then suddenly "extreme pain" at 110'. "Diminishing" from 110' to 50', where the diver realised he was bent.
Now I have no idea what caused the chest pain. While inhaling extremely forcefully? Something to do with the pleural cavity? I have no idea.
Don't want to put words in Don's mouth but his description sounds a lot like radiated nerve pain.
Having herniated 3 disks with associate nerve root compression myself... It seems totally plausible to me that he had a big honking bubble in the spinal epidural space that was compressing one or more nerve roots into the vertebra. That bubble grew, then got compressed, then grew again later as he went up, back down, then finished his deco. Radiated pain from a disk compressing a nerve root is intense, and can be quite distant from the actual nerve root.
First off, thanks for sharing this.
Completely agree. I'd go a bit further about the relevance, though.
We have a diver who experienced two instances of "mild" chest pain in the final stages of his descent. This remained a "minor uncomforting feeling" from 600' to 110'. Then suddenly "extreme pain" at 110'. "Diminishing" from 110' to 50', where the diver realised he was bent.
Now I have no idea what caused the chest pain. While inhaling extremely forcefully? Something to do with the pleural cavity? I have no idea. I does however seem reasonable to imagine that lung function may have become compromised at this point. So offgasing was possibly hindered from 600' to 110', and definitely hindered from 110' to 50', because in addition the diver was now breathing shallow to relieve the pain.
It seems a bit... bizarre to completely ignore all this and focus on the deco model.
Cheers,
Matthieu
Matthieu, I was thinking the same thing. Although it's obviously not a clearly defined indicator of causation, the chest pain during decent and at depth continuing on to 110 feet, seems like to big of a coincidence to just ignore. WOB difficulties during inhalation using an ADV at depth have always scared me and this is one of the reasons why I am a big proponent of having a MAV on both the O2 and Dil side of the unit. I have a hard time imagining that the two issues are not connected in some way! (stated from the safety of my comfortable armchair!)
DSix36
Well-Known Member
Are you suggesting a deeper first stop, slower ascent rate, or both? Why would any GF that is less than 100/100 allow such overpressure, or any overpressure for that matter?I did not show that yet. The profile above is built on the information provided. If you have more details I can add the extra complexities. PM me with the info please.
Your follow up and recovery reads much like a spinal injury. By your own account, the spinal injury aspect was well formed by the time you realized it at 50ft, so this would seem to be an early onset "in water DCS" event.
The area I wish to highlight, is the ascent phase from 600ft to 220 ft, or 11 ATA, and how that over pressure event compares to a USN SurD over-pressure conditions and there limits.
DSix36
Well-Known Member
This actually makes sense too. I previously had neck surgery for a herniated disc and the pain was intense in my shoulder prior to my arm becoming paralyzed from it.Don't want to put words in Don's mouth but his description sounds a lot like radiated nerve pain.
Having herniated 3 disks with associate nerve root compression myself... It seems totally plausible to me that he had a big honking bubble in the spinal epidural space that was compressing one or more nerve roots into the vertebra. That bubble grew, then got compressed, then grew again later as he went up, back down, then finished his deco. Radiated pain from a disk compressing a nerve root is intense, and can be quite distant from the actual nerve root.
- Status
- Not open for further replies.