From your description, you ascended 400ft at 57fpm. That is a lot by any measure or standard. Why did you feel you could avoid the basics of physics that generate bubble growth and injury? Those are well established cause/effect conditions for serious DCS.
The preventive measure to that problem condition, is deeper stops and/or slower ascent rate.
I have to widely agree with ross here just that I get to a bit different conclusions..
To me it seems quite certain that the fast ascent rate plays into it..
But this is not directly related to the choice of model. It actually relates to choice of ascent rate UNTIL first stop and this is double from any recommendation whether you use a bubble model or ZHL + GF..
The recommended implementation of ZHL in combination with Tx is is to NOT exceed 30 fpm (or 10 m/min)..
This is what was learned early and likely prevented DCS cases..
Question is how would the dive have looked like and how would the supersaturations have been if such value was kept and max ascent rate would have been 30fpm plus the 30/90 GF plan..
You followed the plan, and it nearly crippled you. We have not seen this kind of injury level in a long time. I wonder why?
Well I disagree with the statement.. He did not follow the plan, as that would have implied to never exceed 10mpm before the first stop! The outcome might have been very different.
Why not seeing this kind of injury level for a long time? Do you have reliable data about how much dives to such depths have been done at all and then if those dives left over also violated the max 30fpm ascent rule for Tx dives??
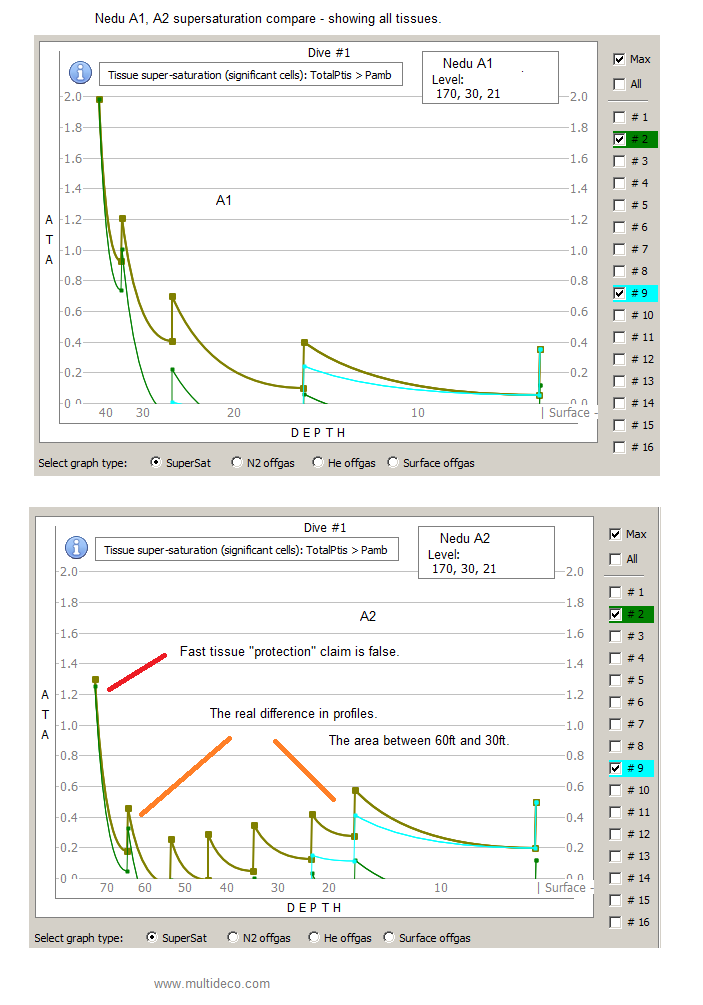
The 60/90 plan has 3 times the amount of supersaturation exposure in water, compared to a VPM-B plan.
Which is the safer plan? Obviously the one that prevents harmful supersaturation pressures from occurring.
Fast tissues do matter, and they will get you injured, as Don has painfully re-discovered.
.
First of all thanks for those comparison graphs they are in fact interesting..
Annoying is again how you try to shape observation in a direction to push your agenda..
The 60/90 "plan" has 3 times the supersaturation.. You cannot call it plan without specifiying the ascent rate limits until first demanded stop.. What you say applies for that fast ascent.. How would it be for max 10mpm?
Which is the safer plan? Comparing apples to oranges as so often..
Obviously the plan with 203 min overall dive time will be the safer plan over the one with 147,5 minutes..
No rocket science there.. how much the distribution of such time impacts the safety is the big question !!
GF 60/90 is horribly agreesive, but not for the GF lo being so high but for the combination of both.. In generally once folks raise their GF lo they should counter with lowering the GF hi in order to keep somehat comparable overall "safety factors".. in my opinion decompression approaches should at cvery first be compared by overall decompression times (starting after leaving bottom!) and only at a second step in how such time is distributed over depth!

 ..
..