Simon, if you would read the links I posted, you would see that it is not just Ross position that NEDU deep stop study was not relevant to our diving, but Bruce Wienke and Marv's too. The profiles (BVM3 and VVAL18) were out of proportion for sport diving.
Hello Igor,
Bruce was present at the Deep Stops workshop and, not surprisingly given that he created the RGBM, he is a proponent of deep stops. Nevertheless, he and just about every other relevant expert in the world were part of the consensus group from which emerged the acknowledgement that the evidence in relation to the relative efficacy of deep stop vs non-deep stop profiles is conflicting.
Since you seem very interested in this issue, why don't we consider the issue of relevance of the NEDU study a little more closely.
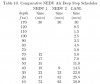
Table 10 (attached below) comes from Bruce Wienke's Deep Stops workshop paper (that is, from Bruce himself). It lists the two NEDU profiles (NEDU 1 = the deep stops profile and NEDU 2 shows the non-deep stops profile) and the RGBM profile (labelled LANL) recommended by Bruce for this dive. As you might expect it has deeper stops than the NEDU deep stops profile. These 3 profiles are then plotted together on the profile figure and the RGBM profile is labelled as B5 (A1 is the NEDU non-deep stops profile, and A2 is the NEDU deep stops profile). This comes from Wayne Gerths' paper (with David Doolette and Keith Gault) at the Deep Stops Workshop. I should point out that there is a minor error in the depiction of the profiles in that the shallowest stop should actually terminate at 195 minutes in the RGBM profile and 206 minutes in the NEDU profiles. The most obvious difference between the NEDU deep stops profile and the RGBM profile is the deeper stops in the RGBM profile.
Now, as a prelude to the rest of the discussion we need to be clear about one thing:
it is tissue supersaturation with inert gas that drives bubble formation. Keep that in mind at all times as you read on.
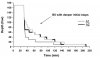
The third figure (also from the Doolette / Gerth paper) labelled T 1/2 = 10 min depicts the tissue supersaturation (expressed in feet of seawater) in a fast tissue (with a short half life) during the decompression according to all 3 profiles. You can see that early in the decompression the NEDU non-deep stop profile (A1) causes the greatest supersaturation in this fast tissue, followed by the NEDU deep stops profile (A2) with the least supersaturation being caused by the RGBM deep stops profile. Thus, the deep stops profiles are doing exactly what they are supposed to do... limit supersaturation in the fast tissues early in the ascent, and the profile with the deepest stops is doing that most effectively.
However, at this point it is worth reflecting once again on the results of the NEDU study. Despite the fact (as you can see from the T1/2 = 10 min figure) that the NEDU deep stop profile (A2) reduced supersaturation in the fast tissue when compared to the non-deep stop profile (A1), the deep stop profile still resulted in a significantly greater incidence of DCS. If reducing supersaturation in fast tissues in the early stages of decompression (which is what deep stops do) was the vital strategy, why would you see a result like that?
This brings us to the final figure labelled T1/2 = 80 min. This depicts the tissue supersaturation (expressed in feet of seawater) in a slower tissue (with a longer half life) during the decompression according to all 3 profiles. What is clear here is that the supersaturations caused by the NEDU non-deep stop profile A1 are smaller and less sustained than either of the deep stop profiles (including RGBM) which are actually quite similar to one another. This supersaturation difference in slower tissues toward the end of the dive between the non-deep stop model and the two deep stop models (including RGBM) is a highly plausible and obvious explanation for the NEDU results which, I would suggest, suddenly don't look so irrelevant.
When this was presented at the workshop there ensued a debate between Bruce Wienke and Wayne Gerth in which Bruce invoked complicated bubble dynamics to explain why you might get a paradoxical result like this, whereas Wayne emphasised the fundamental role of supersaturation in driving bubble formation and observed that the NEDU study showed that emphasising prevention of supersaturation in fast tissues early in the ascent did not seem to be of benefit, especially if that was accompanied by worse supersaturation of slow tissues later in the ascent.
The point I would like to make is that there are very good reasons for not dismissing the NEDU study as "irrelevant" just because the profile did not conform exactly with a typical technical diving bubble model profile. The RGBM profile was not included in the testing program at NEDU so we cannot rule out the possibility that an even greater reduction in supersaturation of fast tissue (depicted in the T1/2 = 10 min figure) early in the decompression might have a beneficial effect later in the dive, but as Gerth would point out, if such a reduction were important, we would have expected to have seen at least some benefit from the reduction (again depicted in the T1/2 = 10 min figure) that was achieved the NEDU deep stop profile (A2) when compared to A1.
So, I suppose I return to my constant refrain. Notwithstanding any weaknesses in the relevant data, virtually all of what is available does NOT support Ross's claim of superiority for bubble model / deep stop approaches (a claim that has absolutely no evidence base of its own) and simply acknowledge what the scientific community have already said: we don't know.
Simon M